
She suggests improvement in the identification and diagnosis of mental health conditions could help to explain the rise. GPs were traditionally found to fail to diagnose up to half of cases of depression or anxiety on initial presentation (Goldberg & Huxley, 1992). Over the longer term, this figure may not be as high or as clinically important as this initial impression may suggest. Some depressed patients are given a diagnosis at subsequent consultations or recover without a GP’s diagnosis. However, there is still a significant minority of patients (Kessler et al., 2002 found 14% in their study) with a diagnosis of persistent depression that is undetected The failure of detection of depression is commonly presumed to arise because of a lack of psychological mindedness amongst doctors. In general, doctors value objective evidence of disease more than subjective experience. This tendency creates a bias towards the over-diagnosis of physical disease, rather than the detection of mental health problems.
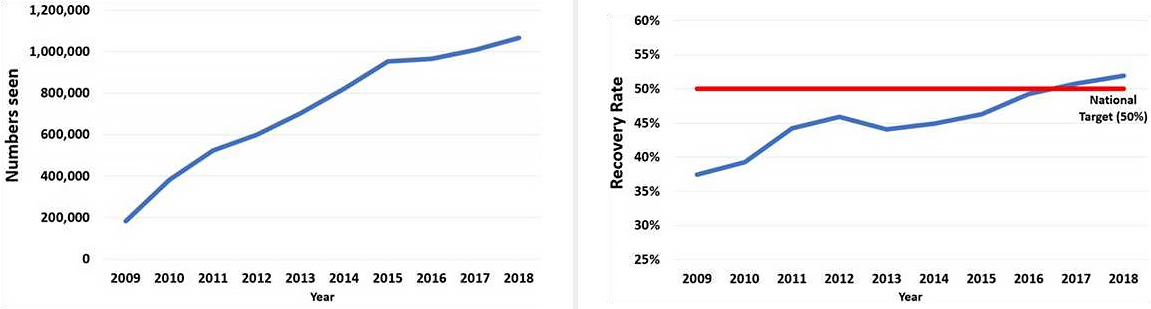
Maybe GPs are now treating and referring more people with anxiety/depression to mental health services, perhaps partly encouraged by the opening up of services by the development of Improving Access to Psychological Therapies (IAPT) over the last 10 years (see graph of increasing numbers of people seen by IAPT) . The number of referrals to general adult mental health services has also increased and figures suggest the number of people seen has more than doubled since 2003, excluding IAPT referrals (see tweet).
Primary care is an essential element of the provision of mental health services and has always traditionally seen more patients with mental health problems than secondary care. Helen Stokes-Lampard complains that access to alternative treatments to medication, such as CBT and talking therapies, is " patchy across the country". She says this despite the introduction of IAPT which was supposed to bridge this gap.
I want to pick up, though, the way in which Helen Stokes-Lampard seems to dichotomise the treatment of mental health problems between medication and talking therapies. In fact, most people seen by secondary mental health services do not receive psychological therapy as such. Even within IAPT, many people do not even receive short-term therapy but instead guided self-help. Polarising treatment between medication and psychological therapy forgets that much mental health treatment is social intervention - helping people understand and recover from the problems with support and becoming as independent as they are able and capable of being. GPs used to do a lot of this work with patients, perhaps particularly when there was continuity of care in general practice. But maybe primary mental health care has become more difficult with the fragmentation and dysfunctionality within health services in general over recent years.
I'm not defending a rise in antidepressant prescribing as Helen Stokes-Lampard could be said to be doing, but I agree with her that these issues - including the role of primary care in mental health treatment - need to be discussed more widely.


{kind=link}